
[Triage Note: Abdominal pain since midnight. Constant. Last BM 15:30 (normal). No diarrhea. Vomiting+. Pain is on right side. Had breakfast (normal). BP 72/58. Pale. Alert. Diaphoretic.]
It’s unusually busy for a mid-summer Wednesday evening. I’ve been called in early for my shift and have been in the E.R. almost two hours. I’ve seen three patients who are contemplating suicide, two elderly patients with chest pain, a young asthmatic, a middle-aged woman with belly pain, a drinker who is vomiting blood, and two people in their nineties who aren’t sure why they’re in the hospital.
I’m sitting at the x-ray monitor at 9 pm when commotion accompanies a stretcher that is rushed into Acute Room #3. His primary nurse, a tall brunette, named Lucinda* asks me to come see the patient. He looks terrible.
Overweight, pale, and sweaty, 55 year old Martin Johnson* is clutching his belly. I ask him what’s been going on as Lucinda completes his vitals. “My wife made meatballs last night,” he says, looking at her. She rolls her eyes – here we go again, it wasn’t the meatballs. “It’s been like this since then.”
“You’ve had this pain since dinner last night?”
“Not since dinner,” he said. “Dinner was fine. It was the leftovers. I had six meatballs around midnight and then the pain.”
“Did you have it all night?”
“I couldn’t sleep.”
I move his hands and palpate his abdomen. He’s sore mostly at the top, over his stomach and his pancreas. His pain follows a line down to his belly-button. There is some tenderness off to the sides as well. He is bloated and has very few bowel sounds. His abdomen isn’t firm, but it isn’t soft either. He winces with each poke. The remainder of his exam – heart, lungs, head, extremities – is normal. There are no skin changes – no marks, no bruises.
“Does it go into your chest?”
“No.” He stops and thinks about it, his knuckles rubbing his sternum. “No. I don’t think so.”
He tells me that he’s never had anything like this before. He’s had heartburn, his wife adds, but nothing like this. He has high blood pressure and high cholesterol – both controlled with medication. He’s had one surgery in his life – a hernia. He smokes half-a-pack a day and drinks occasionally. Apparently he likes meatballs.
“Have you ever been told you have an aneurysm or an ulcer?” I ask.
“No,” they say in unison.
It’s been less than five minutes since I’ve entered the room and I’m scribbling orders on the chart. I’ve called for the portable ultrasound and my assistant has left to find it. “His pressures are unequal,” Lucinda says. “A hundred and five on one side, seventy on the other.”
“I’ll do the scan,” I say, as the machine is wheeled into the room.
Martin is full of gas. I heave blobs of ultrasound gel onto his belly. I ask him to take breaths in and out. He’s too sore to cooperate. I see nothing. Blood is drawn. I order morphine and gravol for his pain. IV lines are placed and fluid is bolused into his veins. I call for a portable x-ray.
The x-ray is complete and on the monitor by 9:20. I study it carefully, hoping to see free air under his diaphragm. I see nothing, and return to the bedside. Lucinda is taking his blood pressure again, and this time she says it with conviction: “Blood pressures unequal, ninety-three systolic on his right arm, and seventy systolic on his left.” Martin’s wife looks for elaboration. Lucinda looks at me.
I tell them what I know, and more importantly, what I don’t know. “I’m not sure what’s causing his pain,” I say. “There are many things that can be causing Martin’s pain. Two worrisome causes for this type of pain are a perforated ulcer, and a bleeding aneurysm.” I point to the x-ray monitor. “Often, if it’s an ulcer, there are signs of perforation on the x-ray, but I don’t see anything. I also couldn’t see anything on the portable ultrasound because there is too much gas in your abdomen.”
“What next?” his wife says.
“The blood work will be back soon,” I say. “If he’s been bleeding since midnight, then his red cell count should be low. Other than that, we’re going to need a CT scan.”
It’s late enough in the evening that I have to page the radiologist. I’m lucky; The radiologist on call is one of our best and she calls me back right away. I discuss the case.
“Okay,” she says. “Creatinine back?”
“No,” I say. “No blood work yet, but he needs contrast.” She agrees. Martin will have contrast infused into his veins. It will be bright on his CT scan and if any contrast leaks out of his blood vessels it will be easy to spot. Similarly, he will drink oral contrast. Any extravasation from his GI tract will suggest perforation of bowel. The contrast is cleared by his kidneys and any impaired function – suggested by an elevation in his creatinine – can be troublesome.
“I’ll call the tech,” she says, “and keep an eye out for his bloodwork.”
I hang up. It’s only been eight minutes since Lucinda has taken Martin’s bilateral blood pressures, but she’s doing it again – left, then right. She calls it out to me again. “Pressures unequal.” She is an excellent, experienced nurse, and we work well together. Usually. But right now, I’m annoyed. I want to ask her – what exactly do you want me to do – but I know what she wants me to do, and at this point, it’s unreasonable. I ignore her. His right arm pressure is over one-hundred systolic – he’s stable for the moment and I have nothing to do but wait for the scan. She documents her concerns regarding the blood pressures, documents that I am aware, and finally, documents that I have given her no further orders. Two minutes later, she will once again document unequal bilateral blood pressures.
Contrast arrives, just as Martin’s blood results are available. There isn’t much to go on: His hemoglobin is slightly low – one hundred and thirty-three. If he’s been bleeding for almost twenty four hours, it should be much lower. In fact, the next patient I’ll see is a thirty-six year old with heavy periods. Her hemoglobin will be eighty-eight.
The department is getting busy. The tech is coming from home and Martin has to chug contrast. Over the next hour, I’ll see seven more patients – two more suicidal, one with a headache, one with retained products from an abortion, a teenager looking for a pregnancy test, a cancer patient with a high fever, and a seven year old I will diagnosis with diabetes.
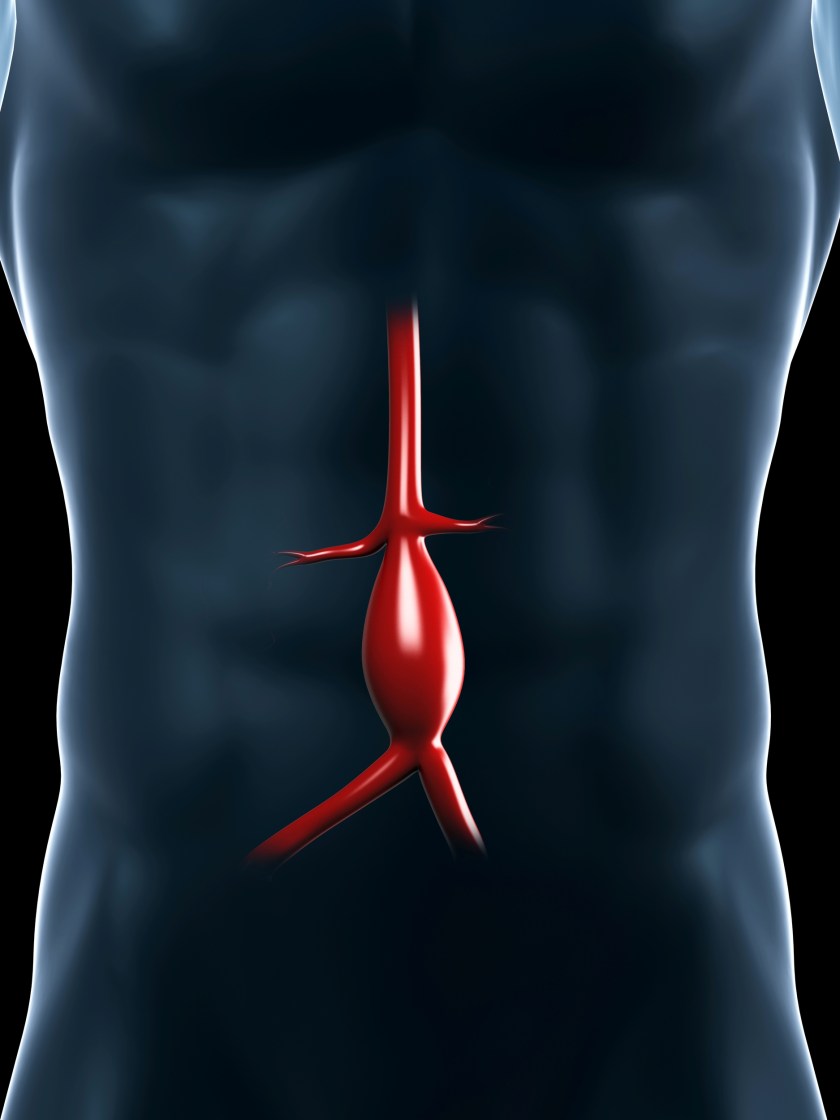
At 10:30 pm, Martin is taken to the scanner. By the time he returns to the department, the radiologist has already called me. Martin is bleeding from his aorta. This is no small leak. His aneurysm is massive. It’s below his kidneys and the size of an egg-plant, hemorrhaging into a bloody collection that is already the size of a football. He needs a vascular surgeon. Fast. At our hospital, we’re lucky enough to have two of them – but unlucky enough to have only two of them. They’re top-notch, but it’s mid-summer and they’re both away on well-deserved breaks. When Martin returns to the department, he looks much worse. He’s grey, his legs are blotchy from lack of blood, his heart rate is rising, and his blood pressure is dropping. I’m already on the phone, discussing the case with Criticall, the province’s emergency transfer service.
I explain the diagnosis to Martin and his wife. He’s hemorrhaging. Fast. He may not survive, and his only chance is urgent transfer to a surgeon who can repair the bleed. It takes a fifteen minutes to make the arrangements, and another fifteen for the transfer crew to arrive. By now, Martin’s receiving potent vasopressors – drugs to raise his blood pressure so that his vital organs – brain, heart, kidneys – remain perfused. Even with these medications, he’s barely hanging on. It will take another fifteen minutes for the crew to prepare for departure and thirty-five minutes – with lights and sirens – to get him where he needs to go. Unmatched blood is transfused. Just before Martin is transferred out, three-and-a-half hours after his initial presentation, the accepting surgeon calls to see if Martin is still alive. I give him the update.
“Make it clear to his wife that there is a good chance he won’t survive, even if he makes it to surgery.”
Lucinda is speaking to Martin’s wife, then she moves to the nursing desk. She tells her colleague, “he should have been sent at the beginning, he had unequal pressures throughout.” It is the case of the evening, and a couple of other nurses gather to see how he’s faring. She tells them the same – the doctor should have transferred him earlier.
I talk to Martin and his wife. They understand the situation’s severity. Just as he’s being wheeled out for transfer, I ask Lucinda. “You think I should have sent him sooner?”
She says it as if it had been concluded hours ago. “He’s bleeding. He had unequal pressures.”
“It means nothing nothing,” I say. “I needed the scan.”
“Well then he should have just had IV contrast. The oral was a waste of time.”
“And if he was an ulcer?”
She’s frustrated with me now. “But he had unequal pressures.” She walks away.
My blood is boiling, but I’m nowhere near finished my shift. It’s busy again and I have patients to see.
I knew it all along, is what Lucinda is thinking, and more dangerously, saying. This is Hindsight Bias. In medicine, Hindsight Bias is dangerous. Psychological scientist Neal Roese of the Kellogg School of Management says, “If you feel like you knew it all along, it means you won’t stop to examine why something really happened.” One of the problems with this particular case is that Lucinda’s initial conclusion – that Martin was hemorrhaging – was based on flawed logic.
Two hours later, after having seen a ninety-five year old on blood thinners who bit his tongue, another nurse, kind, and quiet, asks me why I didn’t send Martin out sooner.
“Based on what.”
“Abdominal pain, unequal low pressures.”
I drew a ‘Y’ on the chart in front of me. I pointed to the stem. “This is where he bled. It was an abdominal aortic aneurysm. Unequal pressures aren’t a sign of a ruptured abdominal aortic aneurysm.”
“Then why did he have unequal pressures?”
“Ask Lucinda,” I said. “She was the one who took them, and she was the one fixated on it.” (See blog on fixation error)
I circled the point of intersection in the middle of the ‘Y’ “Had the bleed been higher up, for example a thoracic aortic dissection, and had it extended into the right subclavian artery, it would have caused a lower pressure on the right.” I circled the first top branch of the ‘Y’. “But this wasn’t a thoracic dissection, there was no involvement of the subclavian vessels, and the unequal blood pressures had no correlation to what was actually happening.”
Only when reviewing the chart for this blog, almost two years later, did I learn exactly how meaningless the declarations of unequal blood pressure really were. True, Lucinda was finding and charting unequal blood pressures, but according to her nursing notes, sometimes the low pressures were on the right, and at other times, the low pressure was on the left. I may approach her one of these days and ask her – what kind of bleed can cause alternating, low, unequal bilateral blood pressures – and how exactly should I explain this to an accepting surgeon.
“Well then couldn’t you have just done the scan quickly with IV contrast instead of waiting for the oral contrast?”
“You’re only asking because you know he was a bleed.”
I told her about a case, that, according to my records, happened exactly seven-hundred-and-fifty days earlier. A sixty-two year old man presented to the ER with severe abdominal pain – epigastric – the same spot and intensity as Martin’s pain. His initial blood pressures were documented as low and unequal – 55/39 on the right, and 70/50 on the left. Three hours after presentation, imaging showed a perforated ulcer. He was taken to the operating room by one of our general surgeons and fared extremely well post-operatively. Yes, Martin needed oral contrast. And hindsight is 20/20.
I was reminded of this case by a letter published in the Canadian Medical Association Journal (187(1)pg.57) this past month. In his letter, a radiologist criticizes a pair of physicians for incorrectly tying unequal bilateral blood pressures to the diagnosis of a ruptured aortic aneurysm (Martin’s diagnosis), confusing this diagnosis with an aortic dissection. Lucinda wasn’t the first one to make this mistake, and probably won’t be the last.
And as for Martin, he survived the transfer to the vascular surgeon, made it through surgery, and recovered to tell the tale.
or, Subscribe to the blog mailing list
*names (and identifying features) of this case have been changed

Great article again Raj! I love reading your blog posts. I wonder if it would be possible to have a monthly talk where the doctors could teach us about the signs and symptoms of different ailments or do a case study so we can learn what to watch for and what certain signs, like unequal blood pressures, mean.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2647165/
An interarm blood pressure differential greater than 20 mm Hg should increase the suspicion of aortic dissection, but it does not rule it in. Significant interarm blood pressure differentials may be found in 20% of people without aortic dissection.