

I have to tilt the rear view mirror downward before I can see him. He’s eight, but still in his booster seat because like me, he’s small. “Hey,” I say. “Do you mind if I run a quick errand after I drop you off at baseball?”
Unlike my eleven year old, he likes me to be there – to watch him – even though he knows I’ll probably give him a hard time if he lets a ground ball slip under his glove. During games, if he makes an error, he looks to the bleachers – for me – and hopes I didn’t see it. “Um,” he says. “Where are you going?”
I wonder whether or not I should tell him. He’s just starting to learn about these things at school. He often jokes about a cartoon from class in which a talking balloon emerges from a trash can to warn kids about cigarettes. “I need to go look at baseball bats,” I say. “I’ll only be gone half an hour.”
“Maybe we can go together,” he says, “after practice.”
“Do you not want me to leave? Because I’m happy to stay.”
“No,” he says. “It’s okay. You go ahead.” He always knows exactly what to say, and how to say it.
“How about this? We’ll go look at bats together after practice. But I have one other quick errand to run. I have to stop by a pharmacy.”
There is a pause, and then he asks. “What do you have to do at the pharmacy?
***
It’s six in the morning, two months earlier, in the darkness of winter. I normally don’t eat breakfast, but when I do this shift, once a month, I’m usually hungry – likely because my body thinks I’m still awake from the night before. The cafeteria isn’t open, and it won’t be for two hours. I’m already cranky when Osler, my assistant, hands me my first chart.
I read the triage note. “Look at this. They made her a three,” I say, referring to her Triage Acuity score, a measure of illness severity. “She should at least be a two. Maybe even a one.”
“Quit complaining,” Osler says. “You haven’t even seen her yet.”
“You should see this triage note!”
“I don’t need to see any note. I saw her when I put her into the exam room. She looks fine.” He taps his watch. “Shut your face and go see her.” This is just like any other day with Osler. I’m sure many of my patients think I’m the one who’s working for him.
When I see her, an IV infusing saline into her right arm, I’m surprised at both how good she looks and how bad she looks. She looks bad because she’s only twenty two and there are dark circles around her eyes and lines on her forehead. She looks at least ten years older than she is. She looks good because an hour earlier, she was unconscious and not breathing. On the exam table beside her, there is a large, disposable cardboard bowl. It’s filled to the brim with a liter of vomit.
As far as puke goes, it’s not that gross. It isn’t creamy, and there are no solid bits or morsels. It looks like Kool-Aid, but has the faint sickly-sweet scent of a second-hand cocktail. The bag of saline is half-empty. She’s received about 500 cc’s of fluid.
“You okay?” I say.
“Ya,” she says quickly. She avoids eye contact. “I’m okay.” She points to the IV. “Can I just get this out and go?”
“Hold on.” Her heart rate on arrival was one-thirty. I put two fingers on her wrist. She doesn’t pull away. It’s settling now, down to about one-ten, one-fifteen. “Do you remember what happened?”
“Ya,” she says.
“So? What happened?”
“I passed out.”
“Why?”
“Fentanyl. First time. Never again.”
“What happened after you passed out? How’d you get here?”
“That’s not important,” she says, her voice a whisper even though the door is closed. “Can I go now?”
I reassure her. “You’re not in trouble. At least let the bag of fluid finish. I’ll give you something for nausea and it will give us a chance to keep an eye on you for an hour or so. The Fentanyl isn’t out of your system yet.”
***
I stay at my son’s practice for the first drill. It’s in a gym and he’s standing about 30 feet from his partner with a ball in hand. He hops toward his partner and launches the ball. It sails fifteen feet over his partner’s head and hits the wall. I squint at him and put my palms up. What the heck was that? He glares back at me. I’ll apologize to him later, when I realize that this was exactly what he was supposed to do – so his partner could field the ball off the wall.
Ten minutes into practice, I leave. The pharmacy is in a strip mall that’s neatly tucked in a new residential neighborhood. There’s a Chinese restaurant on one side, and a dry cleaner on the other. It’s the dinner hour, and thankfully, there’s no one else there. It’s a small town, and the last thing I need is someone who recognizes me, and who doesn’t believe that I’m there for research purposes only.
I introduce myself. He’s been expecting me. He reaches under the shelf and puts two plastic cases on the counter. One has a red cross on it, and the other has a silver one. He shows me a box as well. “You can take these with you if you want,” he says. “I just need a health card.”
“No, no,” I say. “I just wanted to see them first hand. I don’t need to take them with me.”
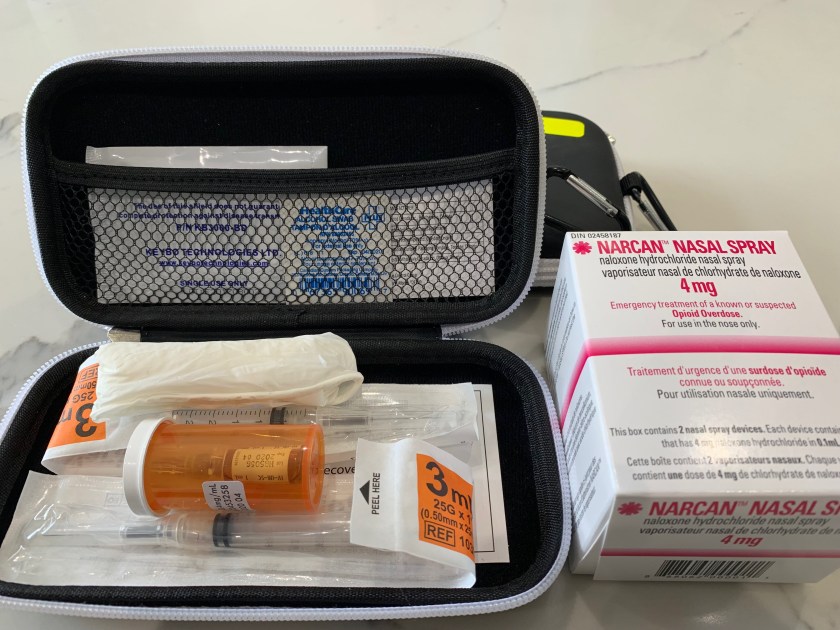
He unzips one of the cases. Inside, there is a see-through pill bottle that contains two tiny vials. Beside this, there is a syringe with a needle attached. There is also an alcohol swab and a rolled up pair of plastic gloves. “This is the needle version,” he says. “But most people opt for the nasal spray.”
“Interesting,” I say. “People who get these kits probably think that the nasal spray is easier to administer and less painful than a needle – which is probably true if you’re giving it to yourself. Not so true if you’re giving it to someone who’s comatose.” He’s about to say something but I cut him off. “And think about the condition the patient might be in. Face down, nostrils filled with vomit, or other secretions. I’d say the needle is the safest way to go.”
“I’ve never thought of that,” the pharmacist says. “The nasal spray is much less intimidating for the general public, so most people choose it.”
***
Two hours later, the cafeteria has finally opened, and I’ve eaten. The cafeteria’s breakfast sandwich – greasy bacon, fried egg, butter, cheddar, salt, pepper – is the world’s best. I’m not cranky anymore. Osler, however, didn’t eat anything. He’s preaching intermittent fasting these days, but will later go home and eat enough of his mother’s homemade kebab to put lamb on the endangered species list.
My patient looks better. There is color in her cheeks. She hasn’t vomited in over an hour. “Can I please go now?” she says.
“Sure,” I say. “But do you remember what happened after you passed out?”
She smiles. “No.”
“What do you remember?”
“I drank a twenty-sixer of vodka with some friends and then someone had Fentanyl.” She doesn’t even remember how she tried it – by mouth, by vein, by nose. “And then, I guess, I passed out.”
“Here’s what happened.” I tell her what the paramedics told the triage nurse. “After the Fentanyl, you lost consciousness and stopped breathing. Your friends started CPR immediately, and someone ran out into the hallway of the apartment building and started screaming out for help. One of your neighbors had a Naloxone Kit. Do you know what that is?”
“No.”
“If someone overdoses on an opioid like Fentanyl or Percocet, Naloxone (or Narcan) will reverse its effects. Whoever gave you that injection probably saved your life.”
“I swear,” she says. “Never again.” She points to the IV. “Now please, can I leave.”
Her heart rate has slowed to one hundred. She’s bright, alert, oriented, and I believe her. She likely won’t do it again after what’s happened today. I could tell her about the dangers of drug and alcohol use, but she’s already learned this first-hand. I can get her to talk to one of our counsellors, but that’ll take another hour, at least. I’m lucky she’s stayed this long. “Do me a favour,” I say. “Stop by a pharmacy and pick up a Naloxone Kit. They’re free*. Even if you’ll never try an opioid again, someone around you might.”
She nods quickly. “Okay, okay,” she says. “So I can go now?”
“Yes.” I say slowly, freezing the moment. “But I’m serious. If you remember just one thing from this visit, remember to go get a Naloxone Kit. All you need is your health card. Tell the friends you were with to get one as well. And you won’t get in trouble for getting one.”
“Okay.”
***
I look through the pharmacy’s windows. We’re in an upper middle-class neighborhood -manicured lawns, two car garages, natural stone walkways. “The people who pick up these kits,” I ask, “where do they come from?”
“Anywhere and everywhere,” he says. He follows my gaze. “This neighborhood, other neighborhoods, mostly locals.”
I think about my own neighborhood. I get at least one call or text every day from friends seeking medical advice. More than once, I’ve had a worried parent knock on my door. I pull out my wallet and hand him my health card. “You know what,” I say. “I think I will take the kit with me. I hope I never need it, but I’ll take it, just in case.”
or, Subscribe to the blog mailing list
* Free in the province of Ontario

Beautifully written
How difficult is it for someone who has never given an injection to inject Naloxone into someone in a crisis?
A Google search brings up lots of links like this one at CBC
Well written as always!!